Pulmonary hamartoma is the most common benign tumor of the lung. It is usually composed of cartilage, fat, smooth muscle and respiratory epithelium. Its diagnosis is based on imaging methods (radiography, computed tomography), and cytohistomorphology study, by means of fine needle aspiration cytology / biopsy (FNAC) or (FNAB).
A 59-year-old female consulted for productive cough and a lung mass on chest radiography. FNA of the nodule showed fusiform tumor cells which was diagnosed as consistent with pulmonary hamartoma (PH). The patient underwent surgery of the tumor mass. The histopathologic study confirmed the diagnosis of PH.
The aspirate from the fluoroscopically guided FNAC was adequate in order to achieve a diagnosis. Cytologic features consisted of a serosanguineous background in which scant cellular elements of spindled and stellate cells, as well as fibromyxoid material enabled us to make a definite diagnosis. Since this technique is relatively non invasive it is very useful in diagnosing PH, preliminarily to any preoperative biopsy.
pulmonary hamartoma ; fine needle aspiration cytology .
Pulmonary hamartoma the most common benign neoplasm of the lung is composed mainly of cartilage, fat, smooth muscle and respiratory epithelium. The majority of these benign lesions are discovered in routinely by chest radiography since the patients are usually asymptomatic. Although the "popcorn" calcification pattern is almost diagnostic by itself, its seen quite rarely (11). The role of FNAC in diagnosing benign lesions of the lung has been thoroughly described in the literature (2,6,10,11,12,13,14). Cytologic findings first described by Dahlgren 1, included spindled and stellate cells with fibromyxoid tissue; cartilage was not present in this aspirate, however, it is considered pathognomonic when present, but nevertheless this key finding is seen only in a minority of cases (2).
A 59-year-old female was referred to our laboratory for diagnostic of a mass in the right middle lobe. She had been smoking about six cigarettes per day for over 20 years. The patient underwent 14 years ago an abdominal hysterectomy and oophorectomy, which were both benign. She complained of a productive cough that persisted for several months. A chest roentgenography demonstrated a round, smooth, well defined lesion in the right middle lobe measuring 2 cm. Computed tomography showed a round nodule of low density with no distant lesions nor lymph nodes affected. Bronchoscopy displayed no pathologic findings. Fluoroscopically guided FNAC of the right lung was performed at our Clinic. The aspirate was performed with a fine 22-gauge needle (10), seven samples were obtained and immediately fixed in alcohol or air dried and stained with Papanicolau or Diff-Quick stains, respectively. The patient was admitted to surgery where a video-thoracoscopy with endoscopic partial resection of the right middle lobe including the nodule was performed. An intraoperative biopsy submitted for surgical pathology (8) was diagnosed as that of PH. Surgical pathology which included cell block histologic sections, confirmed the diagnosis of pulmonary hamartoma without any malignancy.
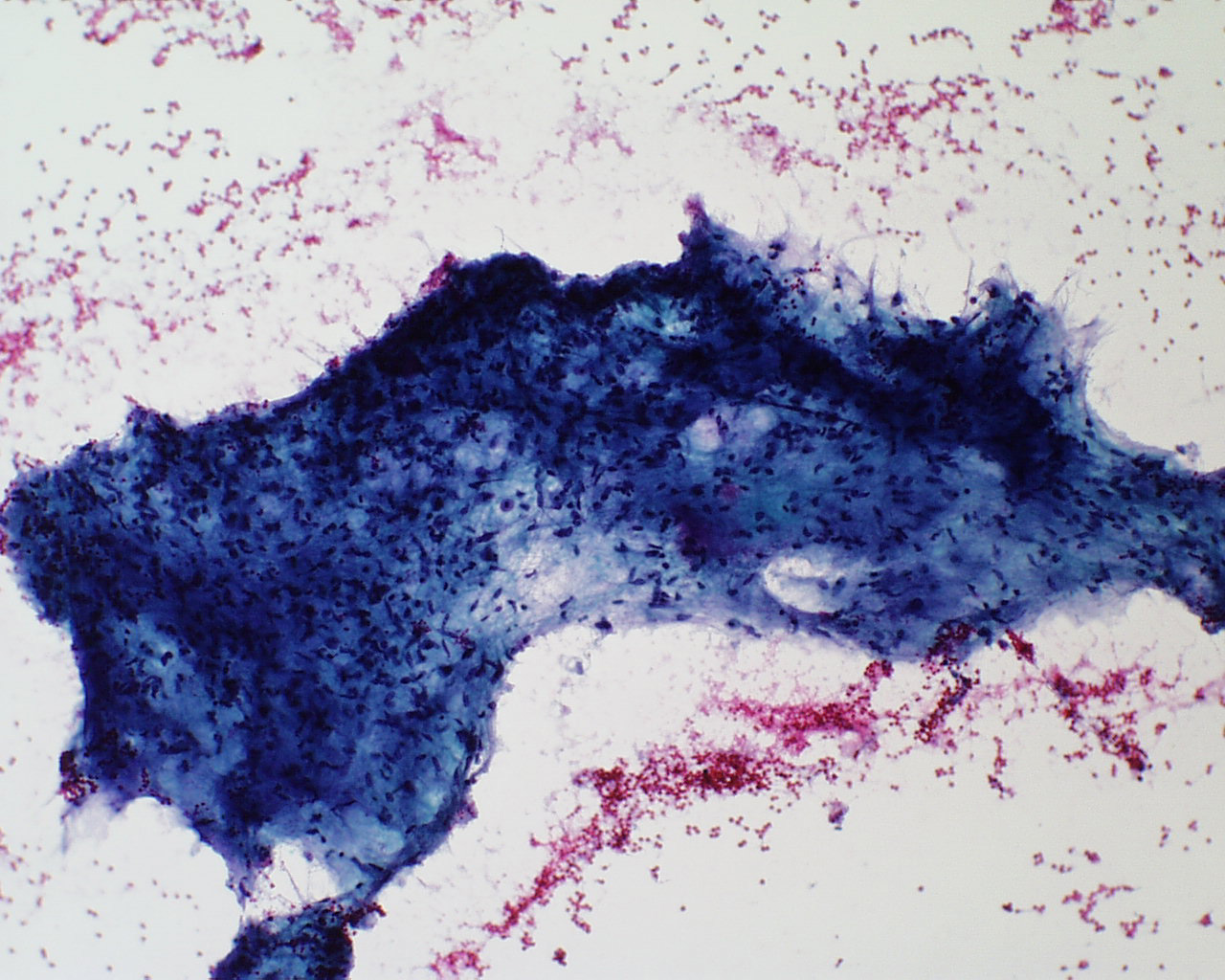
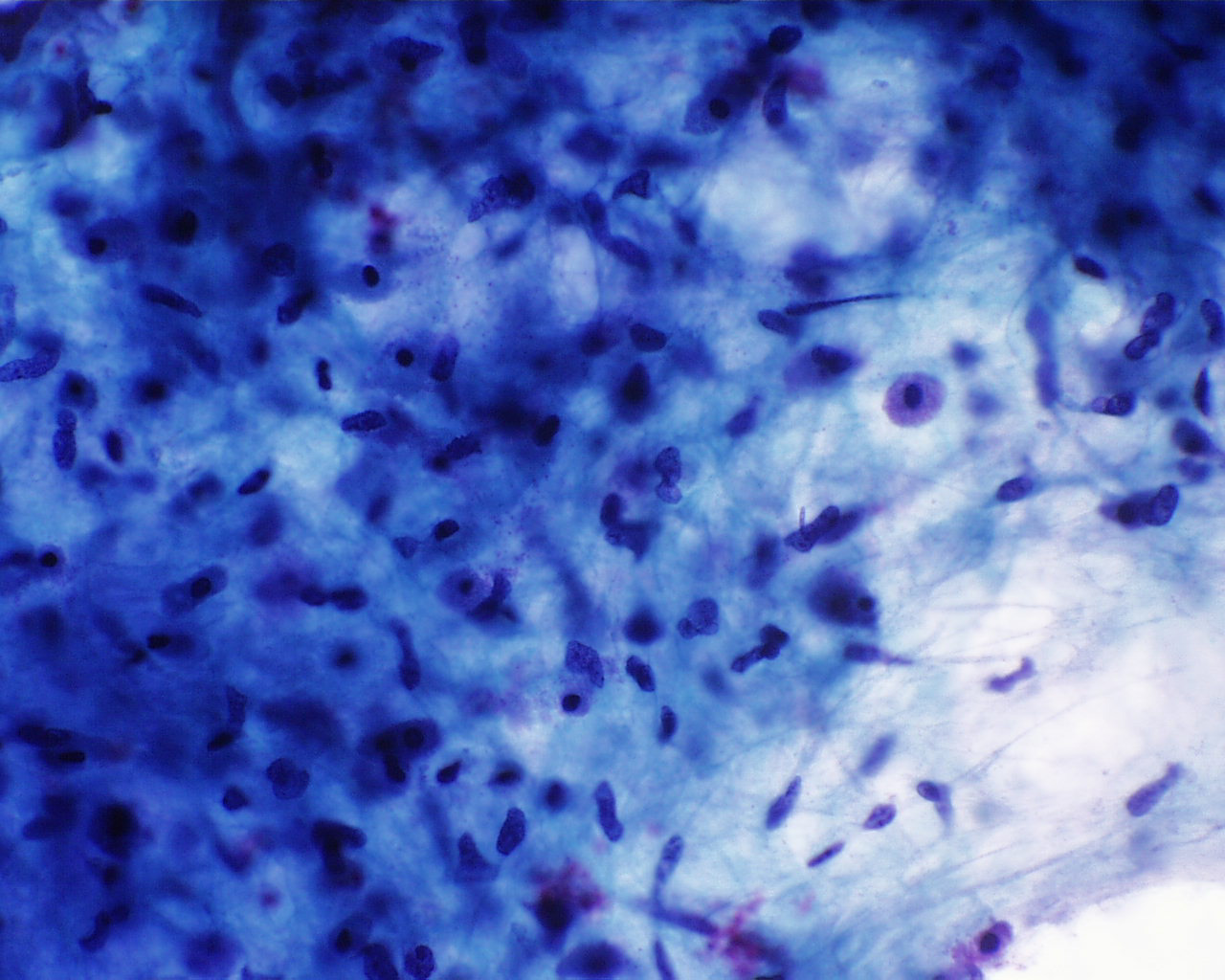
The seven smears contained enough material for diagnosis. The aspirate consisted of serosanguineous background in which scanty cellular material of spindled and stellate cells, as well as fibromyxoid material enabled us to make a diagnosis. Chondroid cellular elements were not found on the smears (Figure 1). The nodule was diagnosed as a fusiform tumor, without broncogenic structures, consistent with PH; nevertheless, loosely arranged cells appeared, that could be suspicious of malignancy, showed variations in nuclear size and isolated cells with nuclear granular chromatin, prominent nucleoli and scanty cytoplasm (Figure 2).
Figure 1: FNA material showing fibromyxoid tissue. Stellate and spindled cells with oval nuclei, notice the lack of cartilage. (Papanicolau stain x 100)
Figure 2: Smear showing a mixture of typical hamartomatous spindled cells and a few bizarre cells with scant cytoplasm, granular chromatin and hyperchromatic nuclei. (Papanicolau stain x 400)
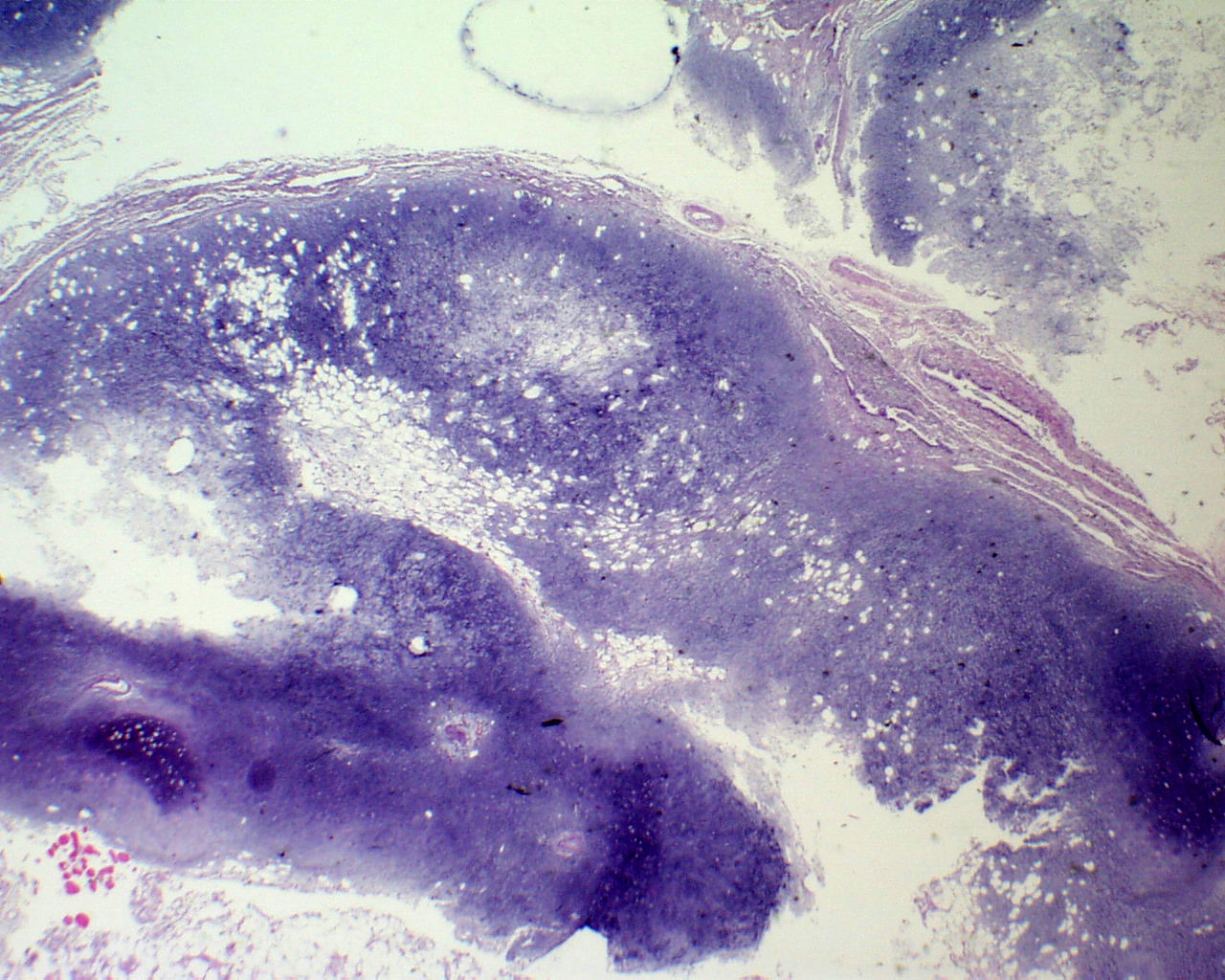
Since the FNAC specimen yielded some doubts about the possibility of malignant findings, removal of the mass was recommended, with further pathologic study. The patient underwent surgery of the lung, ablation of the lesion and wedge resection of healthy pulmonary parenchima. Macroscopically, a well-defined nodule measuring 3 x 2 x 1,3 cm, with a smooth, shiny surface, partially broken and of soft consistency.. The wedge measured 6 x 2 x 1 cm, with no pathologic features noted. Histologically, the resected nodule showed a basophilic stroma with pseudomyxoid and chondroid degenerative changes, covered with respiratory epithelium with deep clefts lined with cuboidal epithelium (Figure 3) The stroma appeared lobulated with a clear chondroid differentiation to well-formed hyaline cartilage (Figure 4) Perinodular tissue showed no special features. The specimen was diagnosed of pulmonary hamartoma.
Figure 3:Typical appearance of pulmonary hamartoma with islands of mature cartilage, adipose tissue, muscle and respiratory epithelium (Papanicolau stain x 20)
Figure 4: Island of mature cartilage. (Papanicolau stain x 120)
Although hamartoma of the lung is a rare benign tumor it is the most common benign lesion of the lung (6,7,8). It presents most times as an asymptomatic mass in chest radiography. Grosly, the cut surface is characterized by ill-defined clefts.
When studying FNAC of a lung mass we tend to look for malignant features. Since it has been aspirated would mean either there exists a clinical suspicion or it has not yet been completely diagnosed by other techniques. Therefore, seven smears were sent to our laboratory from a mass measuring two cm. in which neither radiology nor computed scan could yield a definitive diagnosis. Bronchoscopy and gynecological study found no pathological findings.
Since the smears consisted of scant cellularity, with the previously described cytologic features, in spite of the lack of cartilage, we thought at first of the possibility of pulmonary hamartoma (PH). Nevertheless, the presence of some cellular atypia, nuclei increased in size with irregular thickened nuclear contours and bizarre chromatin aroused us to question the diagnosis of PH and focus our study more on a possible mesenchymal tumor. Acknowledging the benignity of the PH (3,5,9) but possibly in association with a malignant lesion (4,9) forced us to be prudent and advise tumor resection. Later the diagnosis of PH was confirmed histologically as well as its benignity. Therefore, we strongly recommend FNA cytology to diagnose Pulmonary Hamartomas, specially when radiography or computed tomography do not yield definitive diagnosis in a lung mass or nodule. Main importance of this work is to describe a PH without the typical histollogically findings; therefore, increasing the references in this field and help the readers to identify such a findings. Many times this type of lesion is misdiagnosed as lung cancer or tuberculoma by these imaging techniques (15) and the patient undergoes surgery. Hence, the FNAC should be used before any invasive procedure (2, 8,12,14), moreover, considering the low risk of complications by using the 22-gauge needle of FNAC.